A is for Attention-deficit/hyperactivity disorder (ADHD)
Across the globe, around 2%–5% of adults experience symptoms of inattention, impulsivity, and hyperactivity that are connected to attention-deficit/hyperactivity disorder (ADHD) (Staley et al., 2024). With children in the U.S., an estimated 7 million (11.4%) children aged 3–17 years have been diagnosed with ADHD at some point in their life, according to a national survey of parents using data from 2022 (Data and Statistics on ADHD, 2024). ADHD symptoms can vary from person to person, with around 6 in 10 children having specified moderate to severe ADHD. Along with these symptoms, we see that boys (15%) were more likely to be diagnosed with ADHD than girls (8%). We also find that Black children and White children were more often diagnosed with ADHD (both 12%) than Asian children (4%) and that American Indian/Alaska Native children (10%) were also more often diagnosed with ADHD than Asian children (Data and Statistics on ADHD, 2024). Symptoms of ADHD develop during childhood and may continue into adulthood for many individuals.
Many of the characteristics of ADHD are related to what is referred as executive functioning. Executive functioning is the skills we use to manage day-to-day tasks, such as time management, staying organized, regulating our emotions, and planning ahead. While there are several different parts of the brain that contribute to executive functioning, the prefrontal cortex is especially important in regulating these skills. During childhood, the prefrontal cortex is in the process of developing. Because of this development, there is room for some impulsive decisions and hyperactive behaviors that are considered typical among professionals. If you do not know what typical development is though, you will not know what is atypical development. Professionals that are providing therapy to those with ADHD are looking for what is considered atypical behaviors that help assess if a client meets the criteria for an ADHD diagnosis.
What is the DSM criteria for ADHD?
ADHD is considered a Neurodevelopmental Disorder. We have come to learn that people with ADHD have different brain structures, chemical differences, and connectivity changes. For someone to be diagnosed with ADHD, providers must make sure their client is presenting with a certain amount of criteria. This is often seen as certain behaviors within the environment. This process can take on several steps to ensure a proper diagnosis is given as many of these symptoms can also present in other diagnoses, such as trauma responses (ex. high energy, irritability).
During assessments, providers will ask a series of questions to clarify behaviors of clients and move through the criteria. For every diagnosis, client's have to meet a certain number of criteria and not meet criteria for other diagnoses. As an example, we see this in depression vs. bipolar disorder. The DSM criteria does not allow a depression diagnosis to be given if the individual has experienced a manic episode, as mania is not a known symptom of depression but is for bipolar. If there is overlap with symptoms and multiple diagnoses, a provider may not make an ADHD diagnosis during their work with the client in therapy. Many of these client would be referred to a psychologist for ADHD testing where they will complete series of assessments to gather more information on client's functioning. The following is the DSM-5-TR criteria for the diagnosis of attention-deficit/hyperactivity disorder.
ADHD Criteria:
- A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2):
A. Inattention: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required.
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate).
- Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading).
- Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction).
- Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked).
- Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines).
- Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).
- Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
- Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts).
- Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
B. Hyperactivity and impulsivity: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities:
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), at least five symptoms are required.
- Often fidgets with or taps hands or feet or squirms in seat.
- Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place).
- Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless.)
- Often unable to play or engage in leisure activities quietly.
- Is often “on the go,” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with).
- Often talks excessively.
- Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation).
- Often has difficulty waiting his or her turn (e.g., while waiting in line).
- Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
- Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.
- Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g., at home, school, or work; with friends or relatives; in other activities).
- There is clear evidence that the symptoms interfere with, or reduce the quality of social, academic, or occupational functioning.
- The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal).
Specify whether:
F90.2 Combined presentation: If both Criterion A1 (inattention) and Criterion A2 (hyperactivity-impulsivity) are met for the past 6 months.
F90.0 Predominantly inattentive presentation: If Criterion A1 (inattention) is met but Criterion A2 (hyperactivity-impulsivity) is not met for the past 6 months.
F90.1 Predominantly hyperactive/impulsive presentation: If Criterion A2 (hyperactivity-impulsivity) is met and Criterion A1 (inattention) is not met for the past 6 months.
Specify if:
In partial remission: When full criteria were previously met, fewer than the full criteria have been met for the past 6 months, and the symptoms still result in impairment in social, academic, or occupational functioning.
Specify current severity:
Mild: Few, if any, symptoms in excess of those required to make the diagnosis are present, and symptoms result in no more than minor impairments in social or occupational functioning.
Moderate: Symptoms or functional impairment between “mild” and “severe” are present.
Severe: Many symptoms in excess of those required to make the diagnosis, or several symptoms that are particularly severe, are present, or the symptoms result in marked impairment in social or occupational functioning.
Providers assessing for ADHD consider the type of ADHD they are seeing during intakes as it can present in three main different ways: combined, predominantly hyperactive, or predominantly inattentive. They will also identify the severity of the symptoms. This is where we can see different levels of ADHD-type behaviors, appearing to be on an ADHD spectrum. This also shows that individualized treatment will need to be considered for the client and their goals for therapy.
Throughout services, providers are also continuing to assess for any diagnosis that is given to ensure client meets proper criteria for the diagnosis. It is not uncommon for a client's diagnosis to change as providers continue to gather more information and learn more about their clients during the therapy process.
Are ADHD brains really that different?
Simple answer: Yes. ADHD brains are different from an individual with a neurotypical brain. But this doesn't mean their brains are better or worse simply because they are different. Wilkins (2024) discusses that ADHD brains can differ in three ways: the brain structure, brain connectivity, and the neurochemistry of the brain.
Brain Structure
Research has shown for children with ADHD, the prefrontal cortex matures more slowly than typically developing kids. It is also slightly smaller in size. Similarly, the cerebellum, hippocampus, and amygdala are also thought to be smaller in volume in children with ADHD. This shows at childhood, individuals with ADHD have different brain structures.
Brain Connectivity
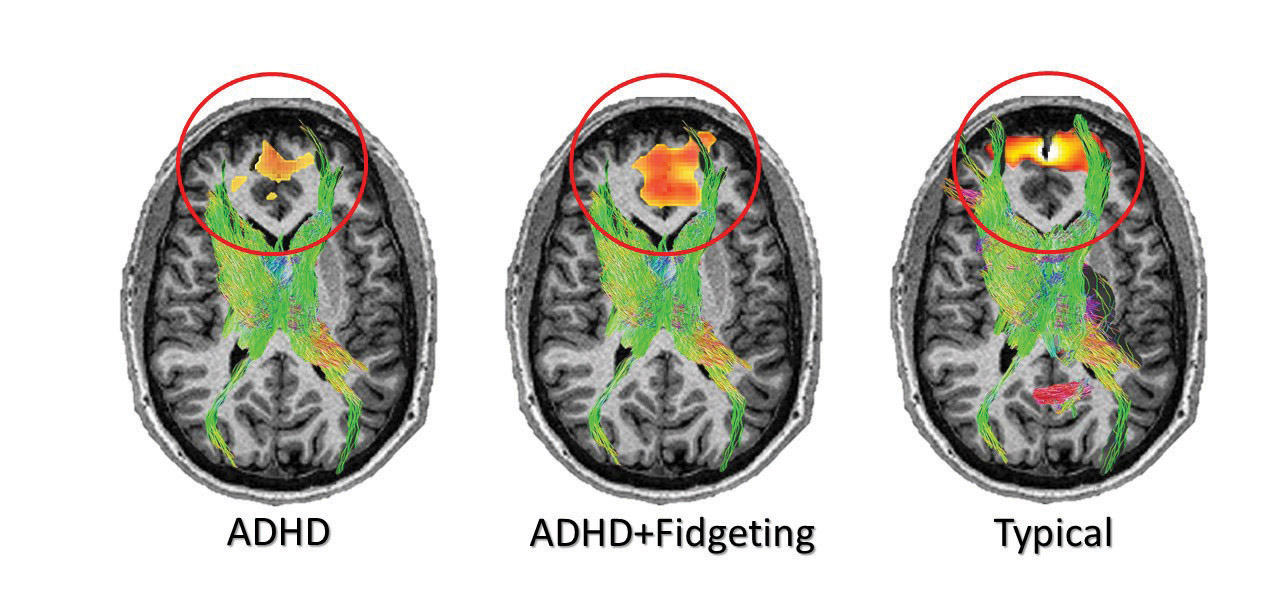
As it relates to connectivity, studies using fMRI technology have shown irregular activity in several regions of the brain involved in motor, cognitive, and emotional regulation.
There is a collective network of structures in the brain that is unusually active in children with ADHD. This is called the default mode network (DMN), and it was first discovered by accident when researchers noticed high levels of brain activity while their study participants were simply resting.
Neurochemistry
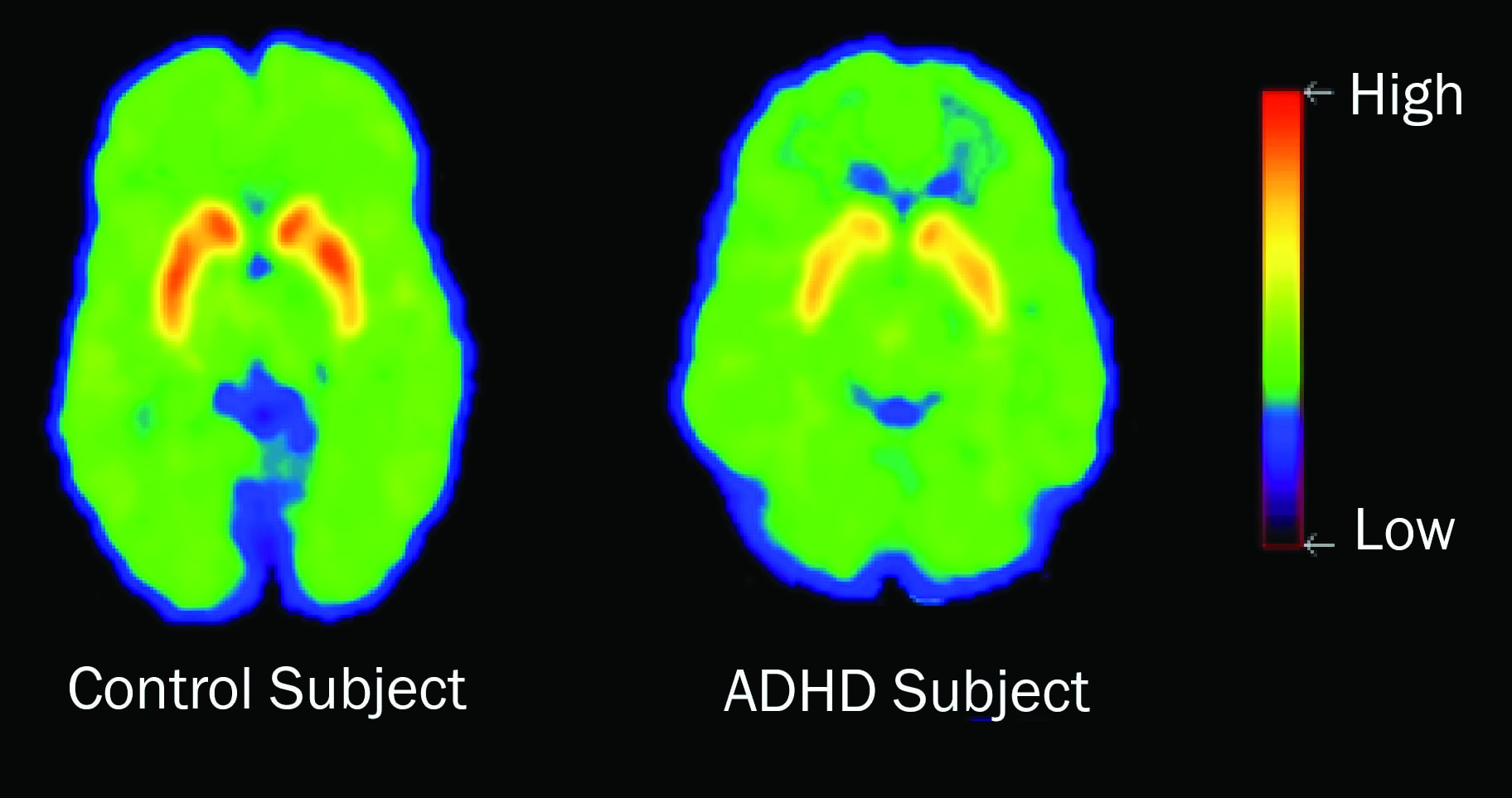
Along with individuals with ADHD have distinct brain structures and connectivity, they also vary in their neurochemistry. The brain controls functions by sending electrical signals through neurons, with neurotransmitters bridging the gaps between them. These neurotransmitters, especially dopamine, play a key role in the brain’s reward system. Dopamine can travel through four major pathways, while two of these pathways are associated with the impairments we see in ADHD.
The two pathways are the dopamine reward pathway and the mesocortical pathway. The dopamine reward pathway is activated by pleasurable experiences, reinforcing behaviors by linking pleasure with memory. The mesocortical pathway connects dopamine-rich areas to our prefrontal cortex, supporting executive functions like memory and decision-making. In ADHD, disruptions in these pathways impair cognition and motivation, making task completion very difficult. One theory suggests there is an abnormal number of dopamine transporters which leads to low dopamine levels. This leads to the need of stimulant medications to block the dopamine reuptake.
Let's Treat ADHD Then!
The types of treatment for ADHD will greatly depend on the presenting concerns for the client. Does this client specifically struggle with inattention? If so, that treatment may be more focused on more behavioral steps such as checklists, using of a planner, and maybe reward charts. Hyperactivity more of the concern? Providers may have these similar techniques but may also incorporate more people to support the client. This could focus on helping with regulation through parent-child interactions, increasing positive interactions and rewards, or potential skills training.
Specifically for working with children, there are several kinds of treatment options of therapy. Parent-Child Interaction Therapy (PCIT), Parent Management Training (PMT), Positive Parenting Program (Triple P) all focus on teaching parents how to use praise, positive reinforcement, and consistent consequences throughout their daily lives, resulting in children being more regulated and redirectable. These treatments often look as though caregivers spending just a few minutes playing with the child, but results show the child is learning they are focused on and important, can rely on their adults, and help the child learn regulation skills through the relationship. These types of therapy result in better behavior from the children such as having a decrease in tantrums, more positive interactions, and resulting in a decrease in parental stress overall (Miller, 2025). These treatments are typically used for younger children. There is less research showing these types of interventions would work for teenagers. With teenagers and adults, the focus of therapy treatment might be a combination of therapies such as Cognitive Behavioral Therapy (CBT) and Behavioral Therapy, along with adding in medication. These therapies may focus more on planning behaviors and charting for clients.
Medications can be an important part of a treatment plan when treating ADHD. There are many options for which medication may work and can also have certain effectiveness for certain people. No matter which medication is chosen though, they effectively work the same way - to increase levels of certain chemicals in your brain, called neurotransmitters. These chemicals help reduce the symptoms of ADHD such as the hyperactivity and inattention, and can increase focus and help manage emotions more easily. Often, ADHD is treated with a stimulant, but these aren't the only types of medication that can work for ADHD. Stimulants are utilized to increase the chemicals of dopamine and norepinephrine, increase the ability to think and pay attention. Common stimulant medications that are used to treat ADHD are Ritalin, Adderall, Concerta, and Vyvanse. Sometimes, stimulants may cause unwanted side affects. Individuals may be recommended to try Nonstimulants for a medication option. These medications may take longer to work but they can help with improving focus and controlling impulses. Antidepressants may also be another form a treatment for ADHD. Although not approved by the FDA for ADHD treatment, some people have found antidepressants can help with symptoms of ADHD. This could be due to the fact that many people diagnosed with ADHD are also dealing with depression, anxiety, or some other mood disorder. These medications may be given together by a doctor in hopes to better improve the use of these medications (ADHD Medication, 2024) overall, as well as help client treat multiple symptoms without multiple medications.
ADHD is a complex and multifaceted disorder that affects individuals in many ways, with its symptoms ranging from inattention to hyperactivity and impulsivity. With the differences in brain structure, connectivity, and neurochemistry may also highlight the need for individualize treatment approaches among those with ADHD. Diagnosis relies on careful assessment based on the DSM criteria, testing, and interviewing to ensure that these symptoms cause disruption to daily life. Treatment, whether behavioral therapy, parent-child interventions, or medication, should be tailored to the specific challenges a person faces. While there is no one-size-fits-all solution, the combination of therapies and medication can significantly improve the lives of those with ADHD, helping them manage symptoms and thrive in their social, academic, and occupational settings.
Individuals with ADHD have many strengths. We often see strengths of extreme creativity, resiliency, and have high levels of courage. Client's may be more able to complete their work tasks at amazing levels and specificity due to their ability to hyper-focus on their areas of interest. Many famous people have an official ADHD diagnosis such as Simone Biles, Emma Watson, and Bill Gates. Many scholars and historians believe that Albert Einstein, one of the greatest minds of all-time, also had ADHD (ADHD Embrace, 2024). Understanding ADHD’s complexities is key to providing the most effective support and fostering an inclusive environment for those living with the condition.

References:
(2024, April 25). The ADHD Brain is Different – Here’s How. Woodburn Pediatric Clinic. https://www.woodburnpediatric.com/blog/the-adhd-brain-is-different-heres-how/
ADHD Embrace. (2024, September 18). Famous People with ADHD - ADHD Embrace. https://adhdembrace.org/famous-people-with-adhd/
ADHD medication. (2024, May 13). WebMD. https://www.webmd.com/add-adhd/adhd-medication-chart
Data and statistics on ADHD. (2024, November 19). Attention-Deficit / Hyperactivity Disorder (ADHD). https://www.cdc.gov/adhd/data/index.html
Invisible Disabilities: The Pathology of ADHD and Autism – Dartmouth Undergraduate Journal of Science. (2009, November 21). https://sites.dartmouth.edu/dujs/2009/11/21/invisible-disabilities-the-pathology-of-adhd-and-autism/
Maude, S. M. (2021, April 14). Study’s MRI images suggest fidgeting good for ADHD brain. New Zealand Doctor Rata Aotearoa. Retrieved May 12, 2025, from https://www.nzdoctor.co.nz/article/print-archive/health-it/studys-mri-images-suggest-fidgeting-good-adhd-brain
Miller, C. (2025, March 5). Behavioral treatments for kids with ADHD. Child Mind Institute. https://childmind.org/article/behavioral-treatments-kids-adhd/
Staley, B. S., Robinson, L. R., Claussen, A. H., Katz, S. M., Danielson, M. L., Summers, A. D., Farr, S. L., Blumberg, S. J., & Tinker, S. C. (2024). Attention-Deficit/Hyperactivity Disorder Diagnosis, Treatment, and Telehealth Use in Adults — National Center for Health Statistics Rapid Surveys System, United States, October–November 2023. MMWR Morbidity and Mortality Weekly Report, 73(40), 890–895. https://doi.org/10.15585/mmwr.mm7340a1
Wilkins, F. (2024, April 10). How is the ADHD brain different? Child Mind Institute. https://childmind.org/article/how-is-the-adhd-brain-different/




